Dr Gautam Tawari is an accredited orthopedic sports surgeon from The Royal College of Surgeon in the UK. Now practising as a Orthopedic Doctor & Surgeon in Mumbai. He has a Diploma in Sports & exercises Medicine (Dip.SEM) from the college and is a Fellow of the Sports & Exercise Medicine Society of the UK.
He has worked as a Consultant Orthopaedic Surgeon in the UK and specialises in advanced elbow joint arthroscopy & Sports related injuries to the elbow joint.
The common sports related injuries he treats surgically include – Tennis Elbow, collateral ligament ruptures, Elbow instability and elbow pain from cartilage damage requiring intervention using elbow Arthroscopy. Sports related elbow fractures / trauma and ligament injuries..

The elbow joint is a hinged joint where the upper arm bone (humerus) meets the two forearm bones (ulna and radius). The unique anatomy of the elbow joint allows it to pass through a broad range of motion. The elbow experiences tremendous stress during repetitive overhead and lifting activities/sports. This may lead to the formation of small loose fragments of cartilage or bone (loose bodies) or elbow joint spurs.
Arthroscopic surgery of the elbow is challenging because of the joint’s anatomy. The bones lie close together, and nerves and blood vessels are located very close to the joint. Although it is a difficult procedure, arthroscopic surgery is often the ideal choice for treating certain elbow conditions. An experienced elbow arthroscopic surgeon can safely navigate through the joint to get the desired results.

An injury or arthritis can damage the ends of the bones and cause bone spurs to develop. These spurs can be painful and make it hard to move the elbow. This extra bone, loose bodies can be removed by using special tools, such as a burr, inserted into the joint through the portals or small incisions. After the spurs are removed, the elbow moves more easily and with less pain.
Conditions like Tennis elbow, OK procedures, Complex fracture / trauma fixation can also be undertaken using arthroscopic techniques.
Operative Procedure Details
An elbow arthroscopy introduces an arthroscope (small ‘telescope’) into the elbow joint through several small 2-3 millimeter incisions.
The arthroscope is used to identify the location of the loose bodies and the spurs.
The loose bodies can be removed by using specially designed small grasping instruments. The bone spurs can be removed by visualising the spur with the arthroscope and using a small burr to remove the spur.
These elbow arthroscopic procedures take about 30-90 minutes and are done as a day-case procedure.

In elbow joint, primary stability is contributed by medial & lateral collateral ligament. The medial collateral ligament (MCL) has three elements the anterior band (which is most important for stability), posterior band and transverse band. The lateral ulna collateral (LUCL) consists of interlacing fibres at different angles and provides dynamic stability to the joint.
Types of Instability
– A traumatic episode disrupts one or more of the elements contributing to stability by placing abnormal forces on to a normal elbow
Chronic/Recurrent – as a result of previous injury one or more of the stabilising elements is deficient and normal forces applied to the abnormal elbow can result in repeated dislocation or subluxation of the elbow.
Treatment
In acute cases, surgery is required to repair anatomical structures to permit active mobilisation of the elbow within a week of the injury if possible. The aim of surgery is to restore and maintain normal articular alignment.
In chronic/recurrent cases, reconstruction of LUCL followed by MCL (if required) is undertaken using either autologous graft (triceps, hamstring or palmaris graft) or artificial ligament (LARS ligament).
Recovery
Active elbow mobilisation is commenced as soon as possible. Stability is improved by undertaking a protocol based phased physiotherapy programme. Return to activities is generally at 4-8 weeks and return to sports at about 3-4 months.
Distal Biceps Rupture
The biceps is a large muscle in the front of the upper arm. It is attached at the top in the shoulder and beyond the elbow into the radius bone by a strong tendon. This strong tendon at the elbow can rupture with a forced contraction of the biceps muscle. It is felt as a pop in the elbow with accompanying pain.
Males over the age of 35 years, strength athletes, bodybuilders or heavy manual workers, are most likely to get a biceps tendon rupture.

Presentation
After the injury there is usually localised pain at the front of the elbow, with bruising and swelling. The biceps muscle may retract up the upper arm crating a prominent bump which is often visibly different to the other biceps when contracting the muscle.
Treatment
Surgery is the mainstay of treatment. A small (percutaneous) approach, reattaching the tendon down to the bone is used. The repair is strong and patients can start moving soon after the surgery in a hinged elbow brace. However lifting must be avoided for at least 6 – 12 weeks weeks after surgery.
Chronic ruptures/delayed presentation
A biceps tendon rupture that is over 4 weeks old is often more difficult to repair directly. The tendon is retracted up the arm and stuck, so a second higher incision may be made to retrieve it. Sometimes a reconstruction with another tendon might also be required.
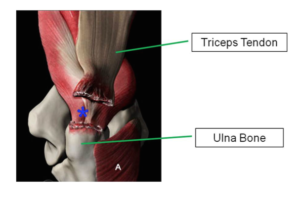
The triceps is the muscle at the back of the elbow . Traumatic distal triceps avulsion is rare and occurs most commonly in contact sports.
Presentation
A history of pain, swelling and bruising at the back of the elbow after a forced flexion in an extended elbow would raise the possibility of triceps avulsion. The strength of elbow extension should be assessed while the examiner feels the tendon for a defect.
Treatment
Surgery is the mainstay of treatment. Anatomical footprint repair for acute ruptures (within three weeks of injury) with transosseous sutures or suture anchors is commonly utilised. For delayed ruptures hamstring grafts taken from the patients own thigh or donor grafts can be used.
Recovery
The elbow is rested in extension splint for 2 weeks and then gradual flexion is allowed. Strength training is started at 6 – 12 weeks.

Tennis elbow is a chronic degenerative condition of the tendon on the outside of the elbow. It is also known as ‘lateral epicondylitis’
Cause
Extensor Carpi Radialis (ECRB) tendon is most commonly affected, and it is usually precipitated by repetitive strain. This tendon is involved in extending the wrist joint and is also active when gripping with the wrist extended (as in tennis). Any activity that twists and extends the wrist can lead to tennis elbow.

Presentation
Tenderness and pain when pressure is applied to the outside of the elbow. Pain when the wrist or hand is straightened (wrist extension) or when lifting a heavy object.
Pain is typically localised over the bony bump on the outside of the elbow (lateral epicondyle) and may extend down to the hand. This area is usually very tender to touch.
Treatment
The type and duration of the treatment depends on the severity of the condition
- Elimination of the activities that cause the pain (tennis, golf, Gym)
- Pain killers medications relieve the pain.
- A tennis elbow clasp can be worn just below the elbow to limit the stress on the ECRB tendon.
- Physiotherapy focussed on the eccentric exercises helps to release the tendon inflammation and retrain the muscles.
- Injections are second line of treatment. Steroid injections should be avoided, they have a detrimental overall effect on the tendon.
- More recentlyPlatelet Rich Plasma (PRP) injections have shown to be more effective than steroid injections, but are more expensive.
Surgery
For very severe cases and those that fail to improve after injections surgery may be necessary. The surgery is usually performed as day case surgery. This may be performed by an open approach, percutaneous or arthroscopically (keyhole).
Prevention
To prevent tennis elbow from reoccurring, it is important to make sure the muscles are kept strong by exercise, warming up before starting to use the muscle may also help to prevent the condition.
Golfer’s elbow is a chronic degeneration of tendon on the inner side of the elbow. It is also known as ‘medial epicondylitis’
Cause
The exact cause of golfers elbow is not known, but it does tend to occur after repetitive strain of the tendon or injury.
Presentation
Pain over the bony prominence on the inner side of the elbow. The pain often extends down the forearm to the wrist and hand. The pain is made worse on loading of the flexor-pronator muscles of the forearm.
Pain is typically localised over the bony bump on the inside of the elbow (medial epicondyle) and may extend down to the hand. This area is usually very tender to touch.
Treatment
The type and duration of the treatment often depends on the severity of the condition.
- Elimination of the activities that cause the pain (tennis, golf, Gym).
- Pain killers and anti-inflammatory medications
- An elbow worn just below the elbow to limit the stress on the muscles helps in initial treatment.
- Physiotherapy focussed on the eccentric exercises helps to release the tendon inflammation and retrain the muscles
- Injections are second line of treatment. Steroid injections should be avoided, they have a detrimental overall effect on the tendon.
- More recently Platelet Rich Plasma (PRP) injections have shown to be more effective than steroid injections, but are more expensive.
If the condition does not respond to the above treatments, surgery may be necessary.
The surgery is usually performed as day case surgery. This may be performed by an open approach, percutaneous or arthroscopically (keyhole).
Prevention
To prevent golfers elbow from reoccurring, it is important to make sure you keep the muscles strong by exercise, warming up before starting to use the muscle also helps to prevent the condition.